Many children are playing the choking game, how large a problem is it, and what is the best way to address it?
Dr Andrew has developed an expertise regarding “asphyxial” games and has presented to a number of audiences. In this presentation he offers some insights into level of the problem but also cautions that teen suicide is a much larger problem.
How should health workers respond? What are the warning signs and how can the problem be best addressed?
Who are children and adolescents who are playing these “games”
Asphixial games have been around for a long time, what differentiates them today is the use of ligatures and solo play. There is a significantly higher risk of fatality when playing alone. It is also harder to determine the manner of death, was it an accident or was it suicide?
These games are known by a by a host of different names including:
| Black Hole | Rush |
| Blackout | Space cowboy |
| Flatlining | Space monkey |
| Funky chicken | Suffocation roulette |
| Gasp | Speed Dreaming |
| Knockout | Tingling |
| Sleeper | Twitching |
| Snuff | Cloud Nine |
| 5 (or 7) Minutes of Heaven | Elevator |
| Airplaning | Hangman |
| Breath Play | Harvey Wallbanger |
| California High | High Riser |
| Choke Out | Natural High |
| Lions and Tigers | Scarf Game (France) |
| Purple Dragon | The American Dream Game (Ireland) |
| Rising Sun |
Why are young people playing these games?
There is a difference between the way that adults and adolescents process information. In an adult processing is performed in the visual cortex or insula. In an adolescent, processing is in the prefrontal cortex, as a result novelty seeking is “hard-wired” in the adolescent brain. Robust developmental changes are still occurring in the insula even at the age of 18.
The question “What we’re you thinking?!”, is a question that many adults may have asked their children at one time, the truth is that they were probably thinking too much! In other words, “It sounded good at the time . . .”
Youth suicide is a bigger problem
It is important to remember that, despite the media response to asphyxial games, youth suicide is a much larger problem. Suicidal violence is annually the second or third most common cause of death in the same age group.
Scene and autopsy findings do not appreciably differ, between a suicide by hanging and an accidental death as a result of solo play in an asphyxial game.
Thorough investigation is the key to accurate certification. Here are some facts regarding teen suicide:
- 78% of youth suicides are male
- Hanging predominates in 11-15 age group and females in general – Though firearms account for nearly as many youth suicides as hanging, overdoses and all other methods combined
- Roughly 22% have made a previous attempt
- 24% were known to have told others of suicidal ideation, nearly 30% had told others of an intent to suicide (3:1 male predominance)
- 51% had “depressive symptoms”
- 32% had been referred for counseling or therapy
- Depression is the most common diagnosis (42%), bipolar disorder was second (14%)
- 90% are medicated
- 30% have had inpatient psychiatric admissions
- Nearly 40% were taking prescribed medication, with 5% on five different drugs at the time of death
- Substance abuse an issue in 60%, but post-mortem toxicology was positive in 32% (excluding intentional overdoses)
- Approximately 60% lived with both parents. 66% of events were at deceased’s residence (including all females)
- 30-40% were experiencing identifiable stressors at the time of the suicide
- Job-related 40%
- Social/relationship 40%
- Legal issues 30%
How is the media responding to the “choking game”?
The media tends to sensationalize the estimates of accidental deaths from asphyxial games, with some media reports suggests that the death toll could be in the thousands, and at least one media outlet suggesting that “Each year, nearly twice as many children unnecessarily die after playing this morbid game than soldiers killed in action in the Iraq War.”
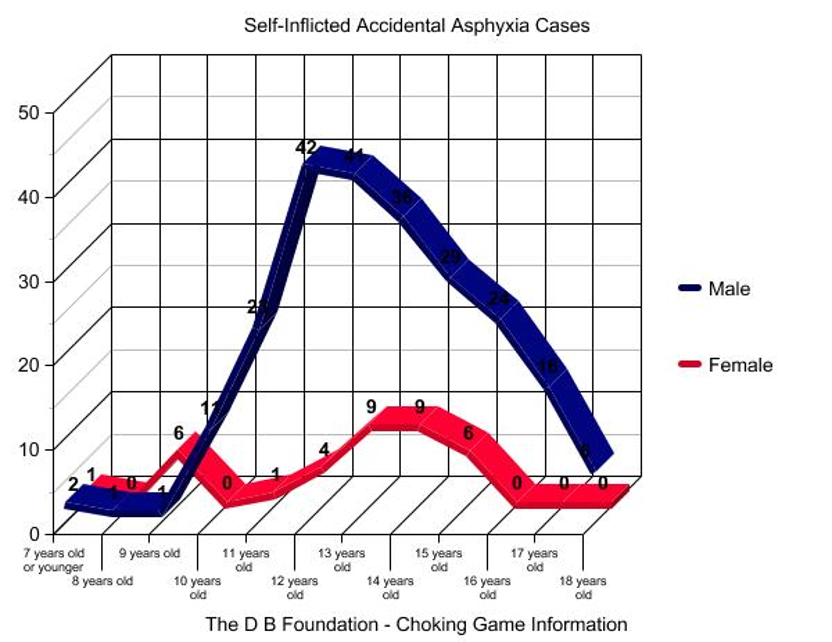
Of course, any death of a young person is tragic, but it is important not to sensationalize the problem too much. The Dylan Blake Foundation, founded by the mother of Dylan Blake to “help establish education programs in schools and spread awareness of a problem too few parents know about until it’s too late.”, has suggested that there are probably less than 100 deaths in the US as a result of these games.
When dealing with the media it is important to avoid sensationalism and not to offer guesses as to the data, and in particular avoid providing information with respect how to do it.
Guidance, warning signs, recommendations
For health care providers, youth counselors and all mentors it is recommended that asphyxial games be treated the same as any other high-risk behavior, to avoid the possibility that it be seen as somehow more exciting or acceptable.
There are several warning signs that may indicate that the young person is engaged in these kinds of games:
For the youth
- Frequent often severe headaches
- Inexplicable bruising or red linear marks around the neck
- Bloodshot eyes and/or petechiae (tiny red dots) on face.
- Changes in attitude (overly aggressive)
- Disorientation and/or grogginess after being alone
- Unusual demands for privacy
- Curiosity about asphyxiation (e.g. “how does it feel?”, “what happens if?”)
Within the Home environment
- Locked or blocked bedroom/bathroom doors
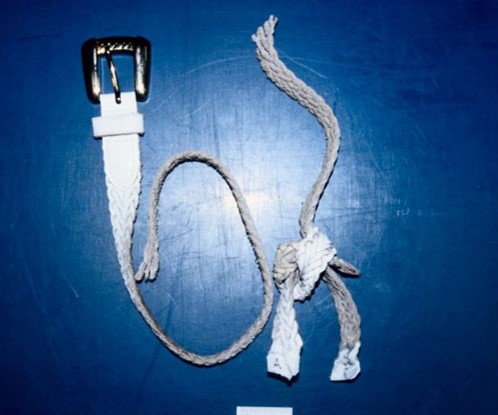
- Ligatures (bed sheets, belts, tee-shirts, ties, ropes) tied in strange knots and/or found in unusual places
- Internet history of websites or chat rooms mentioning asphyxiation or Choking Game
- Wear marks on furniture (ex: bunk beds, closet rods)
Recommendations and Conclusions
The games are not new, but the terms of engagement have changed, solo playing using ligatures in particular. The Internet has made information about these types of activities significantly more accessible.
At the same time suicidal remains a leading cause of death in young adolescents, but some cases may be misclassified because death scenes and autopsy findings involving asphyxial games do not appreciably differ from that found in the case of some suicides.
Investigators must ask the right questions of the right people to expose the possible role of such games in hanging deaths. Clues, albeit subtle, at death scene may suggest unintentional outcome of asphyxial activity, in addition diaries, journals and computers may offer more information
When encountering such cases, providers should engage local resources e.g. public health/injury prevention, pediatric society, youth suicide coalitions and media (judiciously) to raise public awareness.